
Dt. Mahmut Boran
Implantologist & Maxillofacial Surgeon
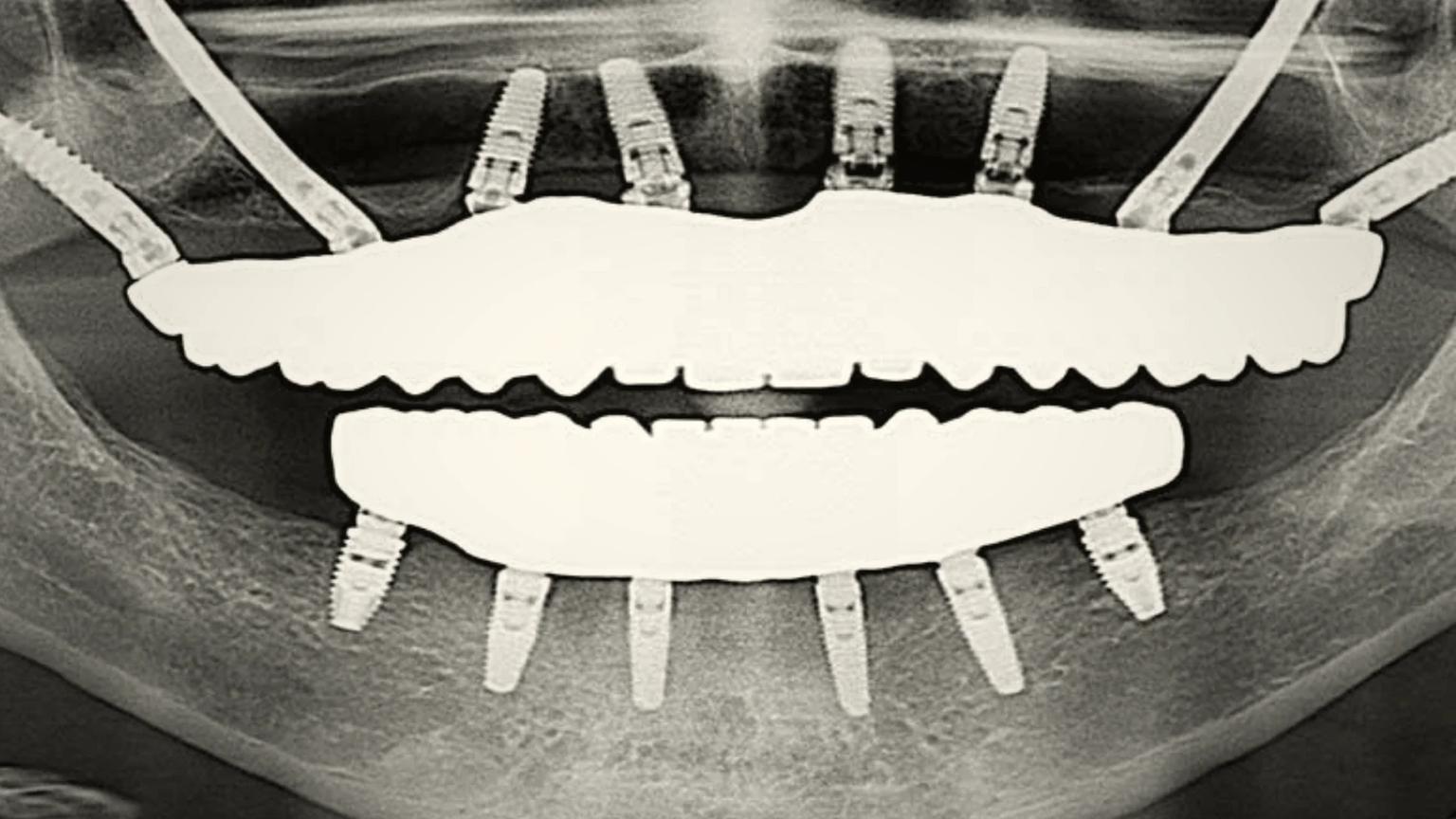
All-on-4 Implant Surgery
- DDS
Zygomatic implant rehabilitation for severely resorbed maxilla, where conventional implants and bone grafting are not viable, performed by a verified partner maxillofacial surgeon and delivered through the ATDERA Care Network of accredited specialist facilities in Turkey, coordinated end-to-end from a UK-registered office.
A verified partner maxillofacial surgeon reviews your case remotely from a CBCT scan covering the maxilla, zygomatic bones, and maxillary sinuses; a panoramic radiograph; clinical photographs; and a full medical history. The review confirms candidacy for zygomatic anchorage, maps the residual bone volume in the zygomatic body and arch, evaluates sinus health, and identifies whether two zygomatic implants per side, a quad-zygoma configuration, or a hybrid plan with conventional anterior implants is the appropriate pathway. ATDERA then issues a written, customised estimate covering the surgeon fee, zygomatic implant brand, immediate-loading prosthesis, anaesthesia, and the in-hospital stay.
On arrival in Turkey, the patient meets the partner maxillofacial surgeon and the anaesthetist for an in-person consultation, intra-oral examination, and digital impression. The pre-operative plan is confirmed against the CBCT data, the implant trajectories through the zygomatic bone are finalised, and a surgical template is reviewed where the case is being performed under guided surgery. Pre-operative blood work and the anaesthetic assessment are completed, and the ATDERA care coordinator confirms the surgical schedule and the post-operative review timeline before admission.
Zygomatic implant placement is performed under IV sedation or general anaesthesia in a hospital operating environment, not under pure local anaesthesia, because the surgical access traverses the maxillary sinus and engages the zygomatic body. The surgeon raises a flap, prepares the implant osteotomy through the maxillary alveolar ridge into the zygomatic bone, and inserts the zygomatic implants — typically two per side — to the manufacturer's torque specification. Where indicated, conventional anterior implants are placed alongside in a hybrid configuration. A temporary fixed prosthesis is attached the same day under the immediate-loading protocol where primary stability allows. The full surgical procedure typically completes within three to five hours per arch.
An overnight in-hospital stay is standard, with a 24-hour post-operative review confirming surgical-site stability, sinus health, and prosthetic occlusion. Soft-tissue healing typically takes two to four weeks, during which mild to moderate swelling at the cheek and upper lip is expected and managed with prescribed analgesics, a chlorhexidine rinse protocol, and prophylactic antibiotics where indicated. Most patients return home within ten to fourteen days of surgery. The ATDERA care coordinator schedules remote video reviews at week 1, week 4, and month 3 with the partner maxillofacial surgeon on file, supported by photographs and any in-country radiographic check the patient's home dentist arranges where appropriate.
Once osseointegration in the zygomatic anchor zones is confirmed by clinical and radiographic assessment, the patient returns to Turkey for fitting of the final e-max or zirconia full-arch prosthesis. This second visit is shorter — typically three to five working days — and ends the surgical phase of the pathway. Annual reviews of zygomatic implant stability, sinus health, occlusion, and oral hygiene are scheduled remotely thereafter through the ATDERA care coordinator, supported where indicated by an in-country CBCT review.
Implantologist & Maxillofacial Surgeon
All-on-4 Implant Surgery
ATDERA does not publish fixed price lists. Every treatment pathway is individually scoped based on clinical review, and costs are discussed transparently once the appropriate pathway, facility, and specialist have been designated for your case.
Join patients from the United Kingdom who have trusted ATDERA to coordinate their Zygomatic Implants internationally.
Share your medical history and treatment goals. We review every case individually.
Our team evaluates your case, confirms suitability, and assigns your named specialist.
We schedule your appointments, coordinate travel logistics, and prepare your treatment plan.
Receive care from your verified clinician at an accredited facility. We manage every detail.
Post-treatment monitoring, discharge planning, and clearance for your return journey.
Scheduled follow-up consultations and coordination with your physician at home.
Ready to take the first step?
No commitment required. Your case is reviewed individually before any referral is made.